|
|
Órgão Oficial de Divulgação Científica da
|
ISSN: 1679-1796
|

Laparoscopic Treatment of a Benign Splenic Cyst
Tratamento Videolaparoscópico de Cisto Esplênico Benigno
Orlando Jorge Martins Torres, Lara Carneiro Lucena, Edem Moura de Matos Junior, Klicia Oliveira Costa, Ana Carolina F. B. Brederodes da Costa, Leandro Henrique Leão Freitas
Department of Surgery - Federal University of Maranhão - UFMA
INTRODUÇÃO: Cisto esplênico é doença incomum na prática cirúrgica diária. O tratamento cirúrgico tem
sido recomendado primariamente para cistos congênitos > que 4 cm para evitar complicações. A abordagem
laparoscópica tem sido utilizada atualmente devido a morbidade da esplenectomia aberta parcial ou total. Este estudo tem por objetivo
apresentar um caso de cisto esplênico benigno tratado por acesso videolaparoscópico. RELATO DO CASO: Paciente de 28 anos, sexo
masculino, sem queixas anteriores, foi admitido apresentando epigastralgia, queimação e saciedade precoce. A tomografia computadorizada
do abdome observou uma grande massa cística dentro do baço. Os exames laboratoriais pré-operatórios estavam normais e o
paciente foi submetido a laparoscopia. A cisto esplênico foi ressecado, retirado através do portal umbilical e enviado para exame histológico.
O período pós-operatório do paciente foi satisfatório e recebeu alta hospitalar após três dias de internação. CONCLUSÃO: A
abordagem laparoscópica do cisto esplênico é um procedimento de baixa morbidade. Proporciona não somente benefícios perioperatórios
distintos, como menos dor e menor tempo de internação hospitalar, mas também resultados efetivos a médio prazo.
Palavras-chave: Cisto esplênico, Laparoscopia, Decapsulação.
BACKGROUND: Splenic cyst is an uncommon disease in everyday surgical practice. Surgical intervention
is recommended primarily for congenital cysts > 4 cm to prevent complications. The laparoscopic approach has
been advocated in recent years due to the morbidity of open total or partial splenectomy. The aim of this study is to present a case
of laparoscopic treatment of a benign splenic cyst. CASE REPORT: A 28-year-old male, in otherwise-excellent health presented
with vague epigastric abdominal pain, heartburn and early satiety. Computerized tomography observed a large cystic mass within
the spleen. All preoperative laboratory tests were normal, and the patient was subject to laparoscopy. The entire extrasplenic cyst was
thus resected, extracted through umbilical port, and sent for histological examination. The postoperative clinical course of the patient
was satisfactory, and was discharged on the third postoperative day. CONCLUSION: Laparoscopic decapsulation of splenic cyst is
a procedure of low morbidity. It provides not only distinct perioperative benefits, including less pain, and shorter hospital stay, but
also effective medium-term results.
Key words: Splenic cyst, Laparoscopy, Decapsulation.
|
Torres OJM, Lucena LC, Matos Junior EM, Costa KO, Costa ACFBB, Freitas LHL. Laparoscopic Treatment of a Benign Splenic Cyst . Rev bras videocir 2006;4(3):118-121. |
||
|
Recebido em 23/10/2006 |
|
Aceito em 06/11/2006 |
plenic cyst is an uncommon disease in everyday surgical practice. They
are classified as either parasitic cysts (hydatid) or nonparasitic cysts, which include true
cysts (primary, epithelial cysts) and false cysts
(secondary, pseudocysts, non-epithelial). Most of the cysts
are asymptomatic, and they are incidental findings during abdominal ultrasonography. The
symptomatic cysts commonly present with abdominal pain,
and there may be palpable splenomegaly or a left
up quadrant mass. Surgical intervention is recommended primarily for congenital cysts > 4
cm to prevent complications such as rupture, hemorrhage, and
infection2,5. Treatment options for nonparasitic splenic cyst include partial
splenectomy, total cystectomy, and decapsulation. Because
open total or partial splenectomy might subject the
patient to considerable morbidity, the laparoscopic
approach has been advocated in recent
years1,6,7. The aim of the present study was to present a case
of laparoscopic cyst decapsulation in the
management of congenital splenic cyst.
CASE REPORT
A 28-year-old male, in otherwise-excellent health presented with vague epigastric
abdominal pain, heartburn and early satiety. Past
medical history was negative, and physical
examination revealed a palpable mass in the left upper
quadrant of the abdomen.
The upper endoscopic evaluation revealed mild gastritis and a computerized
tomography observed a large cystic mass, within the
spleen, measuring approximately 14.0 x 12.0 cm (Figure).
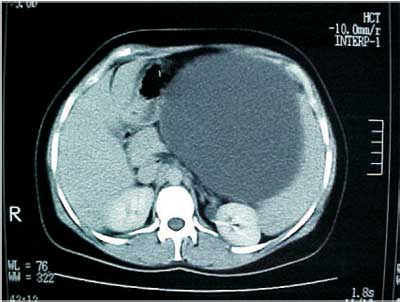 |
Figure: A large cystic mass within the spleen. |
All preoperative laboratory tests were normal, and the patient was subject to laparoscopy.
A 10-mm laparoscopic port was placed in the umbilical position using an open
cut-down technique with direct visualization of
the peritoneum prior to insertion. A 12 mmHg pneumoperitoneum was created, followed
by insertion of a 30° laparoscope connected to a
video system. A thorough inspection of the abdomen revealed a large cyst located along the superior
aspect of the spleen. Three additional ports were
inserted under direct vision. A 10-mm port was placed
parallel to the umbilical port, along the anterior axillary
line. A 5-mm port was placed midline, approximately
5 cm cephaled to the umbilical port. A third port,
5 mm, was placed to the right of midline within
the right upper quadrant. First, the cyst was decompressed via a trocar drainage catheter
inserted into the midportion of the cyst. Approximately
1,500 mL of yellowish serous fluid was evacuated and
sent for cytology and microbiologic study. A scissor
was used to open the extrasplenic cyst from the site
of needle drainage. The cyst wall was excised
using monopolar cautery. The entire extrasplenic cyst
was thus resected, extracted through umbilical port,
and sent for histological examination. The spleen
was inspected for hemostasis. The skin sites were
closed in a subcuticular fashion using a 3.0
Monocryl® suture. Total duration of the procedure
was approximated 95 min.
The patient tolerated the procedure well and postoperative clinical course was
satisfactory, without complications. The patient resumed
oral diet on the first postoperative day, and was discharged on the third postoperative day.
Bacteriological cultures of the fluid were
negative. Histological examination of the cyst revealed a
wall composed of both fibrous tissue and
epithelial elements, consistent with a true cyst. After
six-months follow-up there was no evidence of recurrence or other possible complication.
DISCUSSION
Splenic cyst presents as an asymptomatic abdominal mass or with signs and symptoms of
local compression of adjacent structures. Pain in the
left upper quadrant due to the enlargement and
early satiety are common. Cysts are also discovered
after presentation for the complications of
rupture, infection, or intracystic hemorrhage. They can
be also found incidentally during physical or radiological exam done for other reasons.
Malignant transformation has also been
described2,5.
Pseudocysts were thought to be result of trauma to the spleen with intracapsular
hemorrhage and organization of a fibrous cyst wall.
Importantly, both epithelial and fibrous elements are often
seen histologically within cyst wall specimens
from patients who give a history of trauma.
Computerized tomography (CT) scan is more useful because it
can clearly establish size, position and type of
fluid content; however, the CT examination could
not be diagnostic for the nature of the cyst.
Epithelial cysts are thought to be more common in
younger patients 1,4,3,6,7.
Indications for surgery treatment of splenic cysts include all symptomatic cysts and cysts
larger than 5 cm in diameter. Treatment goals
include elimination of the cyst and prevention of recurrence
1,3,4.
The choice of surgical techniques is of special interest. For a long time, total
splenectomy was considered to be the treatment of choice
for all kinds of splenic lesions, including
nonparasitic cyst. The spleen plays an important
immunologic role, and there is an increasing awareness
of potential early and late complications of splenectomy. The life-long risk of the
development of overwhelming postsplenectomy septic complications has been proven, resulted in a
more conservative attitude in splenic surgery. Preservation of at least 25% of the spleen
offers protection against pneumococcal bacteremia. Treatment options including aspiration, internal
or external marsupialization, partial splenectomy, cystectomy, or partial cyst decapsulation have
been reported and represent the method of choice.
These treatments can be performed by open or laparoscopic surgery
2,3,5,7. More conservative treatments including percutaneous drainage
with ultrasound or CT guidance have not been successful in preventing recurrence, infection,
or bleeding. At present, splenectomy should be performed only when spleen-preserving
techniques are technically not feasible
2,5,6,8.
Splenic cysts may be managed appropriately by partial cystectomy and omental packing.
The method is safe, has minimal risks, and is
associated with a short stay and early return to regular
activity. A potential drawback of this procedure,
whether performed laparoscopically or not, is the risk
of recurrence caused by cyst remnants.
Laparoscopic splenic cystectomy is, however, expected to
prevent cyst-related complications while providing
the necessary pathological
diagnosis1,4,6,7.
The spleen is well visualized laparoscopically. The avoidance of an
upper abdominal incision decreases the postoperative
pain and discomfort for the patient and shortens
length of hospitalization. Laparoscopic surgery provides
a minimal access method to approach small true
cysts of the spleen. In choosing an appropriate
surgical procedure of low morbidity the
laparoscopic approach provides safe, definitive treatment
of benign splenic cysts. In conclusion,
laparoscopic decapsulation of splenic cyst offers not only
distinct perioperative benefits, including less pain,
and shorter hospital stay, but also effective
medium-term results. Thus, the minimally invasive technique should be considered an
advantageous alternative to open
surgery1,4,7,8.
Referências Bibliográficas
1. Calligaris L, Bortul M. Laparoscopic treatment of
a nonparasitic splenic cyst: case report. J Laparoendosc
Surg 1996;6:431-4.
2. Di Carlo I, Fasone MA, Toro A. Epidermoid cyst
of the spleen in the laparoscopic era. Dig Surg
2005;22:53-4.
3. Macheras A, Misiakos EP, Mpistarakis D, Fotiadis
C, Karatzas G. Non-parasitic splenic cysts: a report of
three cases. World J Gastroenterol 2005;11:6884-7.
4. MacKenzie RK, Youngson GG, Mahomed AA. Laparoscopic decapsulation of congenital splenic cysts:
a step forward in splenic preservation. J Pediatr
Surg 2004;39:88-90.
5. Morgenstein L. Nonparasitic splenic cysts:
pathogenesis, classification and treatment. J Am Coll
Surg 2002;194:306-14.
6. Pampaloni F, Valeri A, Mattei R, Presenti L, Nocciolo
B, Tazzini S, Di Lollo S. Laparoscopic decapsulation of
a large epidermoid splenic cyst in a child using
the UltraCision Laparosonic Coagulation Shears.
Pediatr Med Chir 2002;24:59-62.
7. Seshadri PA, Poenaru D, Park A. Laparoscopic
splenic cystectomy: a case report. J Pediatr Surg
1998;133:1439-40.
8. Till H, Schaarschmidt K. Partial
laparoscopic decapsulation of congenital splenic cysts. Surg
Endosc 2004;18:626-8.
ENDEREÇO PARA CORRESPONDÊNCIA
Orlando Torres
Department of Surgery, Federal University of Maranhão
Rua dos Bicudos, 14 apto 600 Ed. Aspen
Renascença II
CEP. 65075-090
São Luís - MA - Brazil
Email: o.torres@uol.com.br