|
|
Órgão Oficial de Divulgação Científica da
|
ISSN: 1679-1796
|

Reparo Laparoscópico de Perfuração do Cólon Durante Colonoscopia
Laparoscopic Repair of Perforation of The Colon During Colonoscopy
Orlando Jorge Martins Torres 1, Everardo de Almeida Nunes 2, Santiago Cirilo Noguera Servin 2, Glayton Stanley Lima Costa 2, Elian Oliveira Barros 2
1Departamento de Cirurgia da Universidade Federal do Maranhão e 2Hospital UDI, São Luís, MA
INTRODUÇÃO: As lesões iatrogênicas do cólon são complicações sérias observadas em associação com colonoscopia
diagnóstica e terapêutica. Estas nem sempre são evitáveis mesmo quando realizadas por profissionais experientes.
Com a finalidade de reduzir a possibilidade de procedimento mais invasivo e evitar o risco de insucesso, a técnica laparoscópica tem sido
utilizada nestas perfurações iatrogênicas. Os autores apresentam um caso de perfuração colônica durante colonoscopia e mucosectomia
tratada com sucesso através do reparo laparoscópico. RELATO DO CASO: Paciente de 46 anos, do sexo feminino, foi submetida a
colonoscopia e mucosectomia. Foi observada uma lesão no cólon transverso que foi produzida pela mucosectomia. A paciente foi então
submetida à laparoscopia e a laceração foi reparada em dois planos de sutura. A recuperação pós-operatória foi rápida e sem
alterações. DISCUSSÃO: Em pacientes com perfuração do cólon relacionada a colonoscopia, consideramos a abordagem laparoscópica
uma opção possível e segura quando realizada por profissionais experientes com o método. O tratamento laparoscópico é capaz de
reduzir o caráter invasivo de uma cirurgia de grande porte. Esta abordagem representa uma excelente forma manusear este tipo de
condição abdominal de emergência.
Palavras-chave: PERFURAÇÃO DO CÓLON; LAPAROSCOPIA; COLONOSCOPIA.
BACKGROUND: Iatrogenic perforations of the colon are serious complications that have been observed in association
with both diagnostic and therapeutic colonoscopies, and are not always avoidable, even in the hands of an experienced
investigator. To reduce the invasiveness of major surgery and avoid the risk of failure, laparoscopic techniques can be done to deal
with iatrogenic colonic perforations. The authors report a case of colonic perforation during diagnostic colonoscopy and mucosectomy
that was treated successfully by laparoscopic repair. CASE REPORT: A 46-year-old woman underwent diagnostic colonoscopic and
mucosectomy. The colonoscopy found a tear in the transverse colon that was produced by mucosectomy. The patient underwent to
laparoscopy and the laceration was repaired laparoscopically in two layers. The postoperative recovery was rapid and uneventful.
DISCUSSION: In patients with perforation of the colon related to colonoscopy, we consider the laparoscopic approach a feasible and
safe option in experienced hands. Laparoscopic treatment seems to reduce the invasiveness and morbidity of major surgery. This
approach represents an excellent means of managing this type of emergency abdominal situation.
Key words: COLON PERFORATION, LAPAROSCOPY, COLONOSCOPY.
|
TORRES OJM, NUNES EA, SERVIN SCN, COSTA GSL, BARROS EO. Reparo Laparoscópico de Perfuração do Cólon Durante Colonoscopia. Rev bras videocir 2005;3(3): 168-170. |
||
|
Recebido em 23/10/2005 |
|
Aceito em 20/11/2005 |
|
|
46-year-old woman underwent diagnostic
colonoscopy and mucosectomy in September
2005 for evaluation of a change in bowel
habits and polypoid lesion. The examination was
performed without difficulty and the mucosectomy was done. It was found during colonoscopy a tear in
the transverse colon that was produced by
mucosectomy (Figure-1). Postprocedure she complained
of diffuse abdominal pain with radiation to
her shoulders. Her abdomen was distended but soft with mild diffuse terderness and no guarding or rebound.
Because of the diffuse tenderness and radiation
of her pain, operative intervention was recommended.
Laparoscopy was discussed and the patient
consented to repair with possible laparotomy.
Our technique employed an open umbilical approach
with one 10-mm, one 10-mm trocar in the left iliac
fossa and two other 5-mm trocars introduced in the
right iliac fossa and right flank under general anesthesia.
A large perforation, measuring approximately
3 cm, was found in the antimesenteric side of the
distal transverse colon. Fecal matter and peritonitis
were not identified in the peritoneal cavity. The
laceration was repaired laparoscopically in two layers:
inner layer with 2-0 polybutylate-coated polyester
(Ethibond, Ethicon, Inc.) running suture and
outer layer with a single 2-0 Ethibond suture. The
abdomen was irrigated with saline and no drain was
used. The nasogastric tube was removed on postoperative
day 2 (after return of bowel function) and
clear fluid diet was started. Antibiotic had been
started preoperatively and was switched to p.o. on
day of discharge, postoperative day 3. Her temperature
and WBCs remained normal. Her laparoscopic
wounds (2-10mm and 2-5mm) healed well without
infection. The postoperative course was unremarkable
and within ten days she was back to office with
no restrictions.
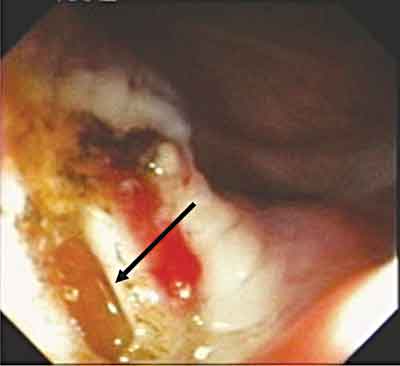 |
| Figure 1 - Tear in the tranverse colon due to colonoscopic mucosectomy. |
DISCUSSION
Colonoscopy is a remarkably safe procedure
with low incidence of major complications such as
bleeding and perforation. The incidence of perforations
has been reported as between 0.045 and 3%.
Diagnostic colonoscopy carries a lower risk of
perfuration, ranging from 0.045 to 0.8%. Therapeutic
colonoscopy carries a risk of perforation ranging
from 0.073 to 3% 2,3,5,9. Although some colonic perforations
are now selectively observed, those that
require exploration and operative repair cause significant
morbidity. Perfurations during therapeutic
colonoscopy usually occurs during hot biopsy or
polypectomy. These perforations are caused by thermal
injury at the operative site and result in a smaller
injury with less contamination than tears from diagnostic
colonoscopy 1,4,5.
Depending on the operative findings and
the skill and experience of the laparoscopic surgeon,
repair may be attempted. Laparoscopic treatment
seems to reduce the invasiveness and morbidity of
major surgery. At the same time, it is more definitive
injury management than conservative treatment.
If laparoscopic repair is possible the benefits
associated with minimally invasive procedures may
be obtained. It allowed us to avoid an unnecessary
laparotomy and other time-consuming and expensive
diagnostic investigations.
Laparoscopy should allow early evaluation
of operative patients and primary repair of those with
minimal surgical contamination and no residual
pathology. Early intervention laparoscopically may
also decrease the severity of this iatrogenic complication
and the need for colostomy and reoperation
for its takedown 2,4,7,8. The benefits of minimally invasive
surgery, such as shortened hospitalization,
more favourable postoperative status and rapid return
to full activities, including work, were realized
in our patient.
FINAL COMMENTS
In patients with an emergency abdomen due
to a postcolonoscopy perforation, we consider the
laparoscopic approach a feasible and safe option to treat colonic perforations in experienced hands. This
approach represents an excellent means of managing
this type of emergency abdominal situation 3,6,8.
Referências Bibliográficas
1. Agresta F, Michelet I, Mainente P,Bedin N. Laparoscopic
management of colonoscopic perforations. Surg Endosc.
2000, 14:592-3.
2. Goh PM, Kum CK, Chia YW, Ti TK. Laparoscopic repair
of perforation of the colon during colonoscopy. Gastrointest
Endosc. 1994, 40:496-7.
3. Ibrahim IM, Sussman B, Wolodiger F, Silvestri F.
Laparoscopic management of iatrogenic colon
perforation. N J Med. 1997, 94:35-7.
4. Mehdi A, Closset J, Gay F, Deviere J, Houben J,
Lambilliotte J. Laparoscopic treatment of a sigmoid
perforation after colonoscopy. Case report and review of
literature. Surg Endosc. 1996, 10:666-7.
5. Miyahara M, Kitano S, Shimoda K, Bandoh T, Chikuba
K, Maeo S, et al. Laparoscopic repair of a colonic
perforation sustained during colonoscopy. Surg Endosc.
1996, 10:352-353.
6. Putcha RV, Burdick JS. Management of iatrogenic
perforation. Gastroenterol Clin North Am. 2003, 32:1289-
309.
7. Schlinkert RT, Rasmussen TE. Laparoscopic repair of
colonoscopic perforations of the colon. J laparoendosc
Surg. 1994, 4:51-54.
8. Velez MA, Riff DS, Mule JM. Laparoscopic repair of a
colonoscopic perforation. Surg Endosc. 1997, 11:387-9.
9. Wullstein C, Koppen M,Gross E. Laparoscopic treatment
of colonic perforations related to colonoscopy. Surg
Endosc. 1999, 13:484-7.
ENDEREÇO PARA CORRESPONDÊNCIA
ORLANDO TORRES
Rua dos Bicudos 14/600 Ed. Aspen
Renascença II
CEP: 65075-090
São Luís - MA
E-mail: o.torres@uol.com.br