|
|
Órgão Oficial de Divulgação Científica da
|
ISSN: 1679-1796
|

Digestive Adaptation with Intestinal Reserve: A New Surgical Proposal for Morbid Obesity
Adaptação Digestiva com Reserva Intestinal: Nova Proposta Cirúrgica para Obesidade Mórbida
Sérgio Santoro1,3, Manoel Carlos Prieto Velhote1,2 Carlos Eduardo Malzoni1 Alexandre Sérgio Gracia Mechenas3 Durval Damiani2 João Gilberto Maksoud2
Hospital Israelita Albert Einstein, São Paulo,
SP1; Instituto da Criança, Hospital das Clínicas da Faculdade de Medicina da
Universidade de São Paulo,
Brasil2; Hospital da Policia Militar do Estado de São Paulo,
SP3 - Brasil
BACKGROUND: Most bariatric surgery techniques include narrow anastomoses, bands or exclusion of
digestive segments, especially duodenum, which is a potential cause of symptoms or complications. This is a preliminary
report on a new surgical technique for obesity: Digestive Adaptation with Intestinal Reserve. METHOD: The technique includes a
sleeve gastrectomy, omentectomy and enterectomy that leaves the first 40 cm of jejunum and the last 260 cm of ileum (totaling three
meters of remnant small bowel). This is within the lower limit of normal range. The digestive reconstruction creates a bipartition in digestive
tract nutrient transit, avoiding the exclusion of segments and prostheses, with the intention of causing minimal to no malabsorption.
Three initial cases are presented. RESULTS: Three patients, two at the age of 16 and one, 39, were operated. With a follow-up of 9, 7
and 5 months, respectively, initial rate of weight loss is satisfactory. Patients are free of symptoms, without diarrhea, referring early
satiety and all of them have metabolic profile improvement. CONCLUSIONS: Early results show that this procedure is capable of provoking
a significant weight loss. However, it does not create obstacles to ingestion of food nor uses prostheses. There are no nutrient
excluded segments, pylorus and duodenum are in transit and there are no blind endoscopic areas. It aims to cause a modest gastric
restriction with early satiety and the procedure intends to modify neuroendocrine response to food ingestion towards a positive change
in metabolic profile.
Key words: OBESITY, GHRELIN, RESISTIN, PAI-1, GLP-1, PYY, VISCERAL FAT, CHOLECYSTOKININ,
OMENTECTOMY, ENTERECTOMY.
INTRODUÇÃO: A maioria das técnicas cirúrgicas bariátricas inclui anastomoses estreitas, bandas ou exclusão
de segmentos digestivos, especialmente do intestino delgado proximal, o que pode causar sintomas e
complicações. Este é um relato inicial de uma nova técnica cirúrgica para tratar obesidade: Adaptação Digestiva com Reserva Intestinal.
MÉTODO: A técnica inclui uma gastrectomia vertical, omentectomia e enterectomia que preserva os primeiros 40 cm de jejuno e os últimos
260 cm de íleo (totalizando 3 m de intestino delgado remanescente). Esta dimensão está no limite inferior da normalidade. A
reconstrução digestiva cria uma bipartição no trânsito de nutrientes no trato digestivo, evitando a exclusão de segmentos e próteses, sem a
intenção de causar má-absorção. Três casos iniciais são apresentados. RESULTADOS: Três pacientes, 2 com 16 anos de idade e 1 com
39 anos foram operados. Com um seguimento de 9, 7 e 5 meses, respectivamente, o ritmo inicial de perda de peso é satisfatório.
Os pacientes estão sem sintomas, sem diarréia, referindo saciedade precoce e todos com melhora do perfil metabólico.
CONCLUSÕES: Os resultados preliminares mostram que este procedimento é capaz de provocar uma perda de peso significante. Entretanto, não
se cria obstáculo à ingestão de alimentos, nem se usa prótese. Não há segmentos exclusos da passagem de nutrientes, o piloro e
o duodeno estão no trânsito e não há áreas fora do alcance endoscópico no trato digestivo alto. O procedimento visa causar
uma adaptação do volume gástrico e modificar a resposta neuro-endócrina à ingestão de alimentos para gerar saciedade precoce
e melhorar o perfil metabólico.
Palavras-chave: OBESIDADE, GRELINA, RESISTINA, PAI-1, GLP-1, PYY, GORDURA VISCERAL,
COLECISTOQUININA, OMENTECTOMIA, ENTERECTOMIA.
|
SANTORO S, VELHOTE MCP, MALZONI CE, MECHENAS ASG, DAMIANI D, MAKSOUD JG. Digestive Adaptation with Intestinal Reserve: A New Surgical Proposal for Morbid Obesity. Rev bras videocir 2004;2(3):130-138. |
||
|
Recebido em 31/08/2004 |
|
Aceito em 06/09/2004 |
besity has become a major public health problem for modern civilization and
many surgical techniques are available, since conservative treatment alone is not sufficient in
a significant proportion of patients. However, all current techniques present some features that
would be better avoided from a strictly physiological
point of view, such as the creation of obstacles to
food ingestion (for examples prostheses or narrow anastomoses), exclusion of digestive tract
segments from nutrient transit and unspecific malabsorption.
Exclusion of digestive segments impedes
endoscopic evaluation of the excluded area and may
cause structural damage to the mucosa, bacterial proliferation and, maybe, bacterial
translocation. Some procedures that involve digestive tract
nutrient exclusion have been related to hepatic
fibrosis1,2, worsening the hepatic condition of patients that
may present with some degree of nonalcoholic fat
liver disease3.
Here, we report three patients submitted
to this new surgical procedure, designed to spare pylorus, duodenum and jejunum from
nutrient exclusion. Indeed, our objective was to avoid
any nutrient exclusion, blind endoscopic areas,
narrow anastomoses and bands.
MATERIAL AND METHODS
This proposed surgical procedure combines many aspects of preexisting procedures, although
it creates a new concept that is the Intestinal
Transit Bipartition. The procedure begins through
a laparoscopic access. Five trocars are positioned:
two 12mm (one in the midline 8 cm above the
umbilicus and the other in the upper left quadrant);
three 5mm trocars (one in the upper right quadrant,
one in the epigastrium for the liver retractor and
one lateral in the upper left quadrant).
First, the omental bursa is opened and section of greater omentum is done with the help
of a harmonic scalpel. Dissection starts just beside
the gastric greater curvature at a point located 6
cm from the pylorus up to the angle of His. A
sleeve gastrectomy is performed with a laparoscopic
linear cutting stapler (Figure 1). A Fouchet's tube is
passed to the stomach to guarantee that the gastric
tube, left in the lesser curvature, is approximately 3
cm wide. The stapling line is covered with 4-0
poly-propylene running suture, interrupted every 4
cm. After that, a 10 to 15 cm midline laparotomy is
made to remove the gastric specimen and the
greater omentum (after detaching it from the colon) and
to perform an enterectomy, leaving the first 40 cm
of jejunum and the last 260 cm of ileum.
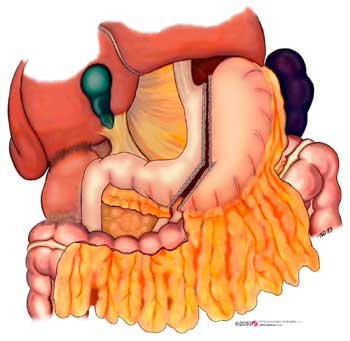 |
| Figure 1 - Diagram showing the proportions of the sleeve gastrectomy. |
Ileum is anastomosed to the lower limit of the stapling line in the stomach, through
the mesocolon (Figures 2 and 3). Jejunum is
laterally anastomosed to the ileum, at 80 cm from
ileocecal valve (Figure 2). The mesenteric borders are
closed to avoid internal hernias. Abdominal wall
and laparoscopic incisions are closed. Antibiotic
and deep vein thrombosis prophylaxes were used in
all patients (cephalothin 1g q6 hours for one day; enoxiparin 60 mg once daily, preoperatively and
for two weeks after the procedure).
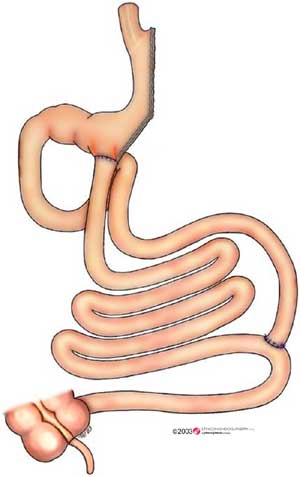 |
| Figure 2 - General aspect of the Digestive Tract after the procedure. |
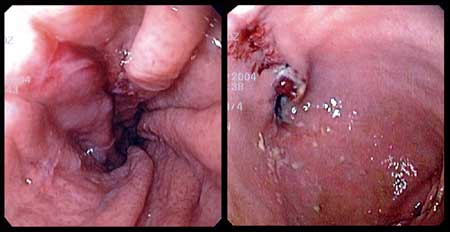 |
| Figure 3 - Two endoscopic views: Left - proportions of the sleeve gastrectomy; Right - pylorus (right lower corner) and ileo-gastrostomy at the end of the stapled suture (left upper quadrant). |
The Ethical Committee of the Hospital
da Policia Militar do Estado de São
Paulo approved the protocol. The procedure was reviewed and
also accepted at the Instituto da Criança do Hospital
das Clínicas da Faculdade de Medicina da Universidade
de São Paulo. A detailed informed consent was
signed by patients or by responsible relatives.
PATIENTS
CASE 1 - Female, 16y; weight 137 Kg (height 158 cm; Body Mass Index 54.9
Kg/m2). Although very young, she presented with
systemic arterial hypertension and insulin resistance
(glucose/insulin ratio = 2.0). She was operated on
October 2003. Presently, she refers early and intense
satiety. Hunger became an infrequent sensation and,
in some periods, she ate even less than that
expected by the medical team. She no longer presents
systemic hypertension and is symptom free.
She has lost weight efficiently. She
weighed 88 kg in April 2004. Her fasting glucose is
normal (78 mg/dl) and fasting insulin is 21.8
mIU/ml (glucose/Insulin ratio = 3.8 indicative of
improve-ment in insulin resistance). At the end of July,
2004 she weights 75 Kg (62 kg lost in 10 months)
CASE 2 - Male, 16y; weight was 219
Kg (height 175cm; Body Mass Index 71.5 Kg/m2). Although very heavy, he did not
present comorbidities. He was operated on December
2003. He presented an intraabdominal infection
that required surgical drainage, but no dehiscence
or fistula was detected. Now he is also symptom
free and presents early and prolonged satiety. His
bowel movements became more frequent (twice,
sometimes three times a day), but liquid feces have not
been observed. Now he weights 140 Kg (79 Kg lost in
9 months). Blood tests, as before, continue
normal. He is still loosing weight.
CASE 3 - Female, 39y, weight was 146
Kg (height 161 cm; Body Mass Index 56.3 Kg/m2).
She presented arterial systemic hypertension, hypertriglyceridemia (267 mg/dl) and
hypercholes-terolemia (299 mg/dl). She was operated in
February, 2004. Due to a very large fatty liver, the
laparotomy was done with a transverse incision. After
five months, she is symptom free. Her bowel
movements are a little less frequent (once every two days)
and she lost 41 kg in 5 months. Total cholesterol fell
to 168 mg/dl and triglycerides fell to 136 mg/dl.
She does not take antihypertensive drugs anymore.
The surgical procedures took from 200 to 290 min. All patients resumed taking oral liquids
in the second post-operative day and they were
advised to maintain only a liquid diet for seven days
and then resume solid foods. Omeprazol, 20 mg per
day and polyvitamin pills are initially
recommended, since the amount eaten may be low enough
to generate deficiencies.
After two months, radiological studies
show that the main part of the ingested contrast
follows the gastroenterostomy route, but also a
significant part passes through the pylorus. Patients do not
report any worsening neither in flatulence nor in the
feces odor. All three patients expressed satisfaction
with the procedure.
DISCUSSION
We have recently hypothesized that the
long length of human small bowel, especially jejunum,
is an evolutionary remnant and is not adapted to a modern
diet4. Primitive diet was hypocaloric
and full of poorly digestible fiber. A primitive
human would have to ingest large food volumes to
obtain just a small amount of calories. Also, it is hard
to extract nutrients from the bulky non-nutritive particles and to absorb them. A large stomach
and a long bowel are important as containers, but
they also provide the opportunity for absorption of
all nutrients among the fiber and indigestible
particles. On this diet, nutrients would reach distal parts
more easily.
Modern diet has concentrated, highly absorbable nutrients (including unnatural
elements such as refined sugar and white flour) and
with progressively less fiber and residues. It is possible
to efficiently absorb these in the very first portions
of the intestine, thereby creating peaks of
nutrient absorption and an "empty distal gut".
Nutrient-induced secretion of enterohormones produced
by the distal bowel would be attenuated in this scenario.
Glucagon-like peptide 1 (GLP-1) is a polypeptide hormone that is secreted from
the enteroendocrine L-cells of the distal gut in
response to nutrient ingestion5. It has five
fundamental actions. First, it causes potent stimulation of
insulin biosynthesis and release from pancreatic
beta-cells (potent enough to potentially cure type II
diabetes)6. Second, it reduces gastric acid
output7 . Third, it causes major reduction in gastric
emptying8. Fourth, it causes relaxation of the gastric fundus,
allowing the stomach to contain a larger volume
without increase in distension
sensation9. Finally, GLP-1 goes beyond the blood brain barrier and causes
satiety10. The evolutionary aspects of the GLP-1 functions
are fascinating. Because of sporadic access to food
in Nature, primitive man instinctively ate as much
as possible to create reserves for periods of
hunger. While he is hungry during a meal, the
digestive transit must be fast to create space for further
eating, but, when nutrients reach the distal gut,
intestinal transit must be slowed, otherwise nutrients
could be lost in stools. The secretion of GLP-1 by the
distal gut controls the entire process slowing
gastric emptying, provoking intense insulin secretion to
help the organism stock absorbed nutrients inside
the cells, relaxing the gastric fundus to let it
contain the food that cannot be processed straight
away, causing central satiety to stop eating and
diminishing gastric acid output, since the meal is about to finish.
Polypeptide YY (PYY) is also a gut hormone
involved in the response to food ingestion. It belongs to
the pancreatic polypeptide (PP) family along with
PP and neuropeptide Y, and it is found in two
forms PYY1-36 and PYY3-36.
PYY3-36 is more specific to Y2 receptors in
hypothalamus11. It is released, also,
by L cells in the gut in response to food ingestion
and it causes saciety12.
Oxyntomodulin is another polypeptide hormone that is generated by processing
proglucagon molecule and is secreted after nutrients reach
the small bowel; it reduces food intake and
appetite13 and is also involved in the gut-to-brain signaling.
If the presented theory is correct, two
facts would have to be proven: first, that obese people
do have attenuated secretion of distal bowel
hormones; second that obese people are able to produce
them adequately, if enough nutrients reach distal gut.
Both facts have already been demonstrated.
Obese14 as well as type II
diabetic15 individuals have attenuated postprandial GLP-1 secretion.
Also, immediately and many years after a
jejuno-ileal bypass is performed (which throws nutrients to
distal gut through a shortcut), normal GLP-1 secretion
is reestablished16. A bowel resection can do the same.
In summary, to have 3 or 8 meters of small bowel (lengths eventually found in normal
and never-operated-on persons) makes little
difference in terms of absorption, since in neither
case malabsorption will occur. However, it seems
clear that to have nutrients reaching and being
absorbed by the distal gut is an important physiological
issue, especially in limiting food intake, through
the production of intestinal hormones that work as
signs to the pancreas and to the brain.
Following this line of reasoning, we could go still further. Obesity has been related to
increased incidence of colon cancer17. Nutrients
reaching distal gut provoke secretion of GLP-2 and
generation of short-chain fatty acids (SCFA) in the colon.
Both, GLP-2 and SCFA are thought to be protective against colon
cancer18,19. So, scarcity of nutrients
in distal gut could link colon cancer and obesity.
Both conditions have parallel increasing incidences.
These data suggest that, especially if modern, hypercaloric, easily digestible diet is
being used, it might be better to be "normal with 3
meters" than to be "normal with 8 meters" of small
bowel. Could the length of small bowel be involved
in obesity? Do the obese have longer small bowel?
There have been few studies into this matter, but the
article by HOUNNOU G et al.20, proposes that this is
the case.
Evolutionary forces have been at work in this matter. Early hominid species were
herbivores. During the process of becoming omnivorous,
the higher concentration of calories in the meat
and the better foraging strategies allowed these
Homo groups to eat less volume of more digestible food.
It is known that in these transitions the amount
of bowel was reduced21,22 (as expected, since
exclusively herbivores have longer bowel extensions).
During the last century, another great change occurred in human diet, which became
more concentrated in calories and even freer of
non-digestible particles, which has led us to
consider that a further bowel reduction is now
necessary. Evolution continues to perform its timeless
job: natural selection. People are becoming obese
and dying. Obese people, as HOUNNOU G et
al.20 pointed out, have a longer bowel, and thus
shorter bowel is being selected.
The "contemporary human being"
is insufficiently adapted to the abundance of
easily absorbable food, which is causing a lack of
nutrients in distal bowel with serious endocrine and
metabolic consequences.
Faced with this modern diet, our small
bowel has become inappropriately long and
excessively permeable, and likewise, the stomach, as a
storage chamber, is too large. In parallel, our eating
instincts are upregulated while daily physical effort
has diminished. Obesity, hypertension,
dyslipidemia, atherothrombosis, diabetes are some of
the consequences.
Based in this rationale, we recently described a new surgical strategy to treat
obesity: Digestive Adaptation23 (Figure 4). It is composed
of a vertical (sleeve) gastrectomy, omentectomy and
a simple enterectomy that leaves 3 meters of small bowel (1.5 m of jejunum and 1.5 m of ileum).
The gastrectomy aims to adapt the size of gastric
chamber to the high caloric-dense modern
diet24, reducing its volume. Satiety signs caused by distension
will be emitted earlier and the main source of
ghrelin25,26,27, a gastric orexigenic hormone,
is removed. The enterectomy does not aim to create malabsorption (this remnant length is in the
lower limit of normal range and sufficient to
complete absorption and still with functional reserve). It
is performed to adapt the small bowel to modern
diet and to adequate intestinal hormonal responses
to food ingestion.
It is a physiological approach and twenty-month results with Digestive
Adaptation23, including more than 50 patients, operated in several
centers by many other surgeons utilizing the same technique, are very good (in press). However,
in patients with BMI greater than 45 Kg/m2, with severe comorbidities, an even shorter bowel (40
cm of jejunum and 80 cm of ileum) would probably
be more appropriate. Nonetheless, it would not be
wise to perform such an extensive enterectomy
because the patient would be left without a
functional reserve. This motivated the development of
the technical alternative, presented here.
It seems that, as a procedure to treat
morbid obesity, it might be superior to other
alternatives because it does not involve obstacles to
food ingestion, the pylorus remain intact, and
duodenum is in transit, so able to develop its special
absorptive and neuroendocrine functions. There are
no segments excluded from nutrients transit, nor
from the access of an endoscope. Furthermore, it is
easier to perform, with fewer risky steps. There is
neither manipulation of gastric lesser curvature nor the
need to adapt prosthesis. The anastomoses involved
are easier since they do not involve the duodenum
or high pouches in the stomach.
An amount of food goes through the
pylorus. This route resembles the jejuno-ileal bypass used
in the past28. However, the route is longer (120 cm
post Treitz) to reduce malabsorption (or avoid it in
the long term) and this is compensated by a
smaller gastric capacity. Also, the absence of an
excluded segment may avoid complications such as
hepatic fibrosis and cirrhosis29,30.
Some food passes through the gastro-enterostomy. This will meet a 1.8
meter-long segment of ileum, without (or little)
biliopancreatic juice and after that, receive the digestive
juices through the enteroenterostomy, and then
follow through the terminal ileum. This route is similar
to that found in a biliopancreatic bypass.
Radiological studies have shown that after two months, the preferential path is through
the gastroenterostomy. However the duodenum is not excluded; its nutrient stimulation may generate
its unique hormonal and absorptive response (at
least with a part of the meal). Besides the functional
gain, it probably will prevent bacterial proliferation
and translocation to portal blood, preventing
hepatic fibrosis as a consequence; also having all
segments in transit might be the reason why none of
these patients observed diarrhea, worsening in the
odor of feces or in flatulence. This is an important
issue when we aim to afford these patients a better
social life and improved self-esteem. In summary, it
was avoided a non-physiological feature such as
nutrient exclusion.
Regarding the improvement in the metabolic profile, the proposed technique may
help. Indeed, whatever path the food takes, nutrients
will reach distal bowel in larger amounts than
they naturally would. Nutrients in distal gut provoke
the secretion of GLP-131. Early and effective
elevation of secretion of GLP-1 can cause a delay in
gastric emptying, central satiety, intense stimulus
to trophism of beta pancreatic cells and a strong
insulin secretion that can result in the cure of type
II diabetes5. Secretion of PYY and
Oxyntomodulin, also provoked by luminal nutrients,
enhance satiety12,13.
The procedure intends to enhance postprandial secretion of Cholecystokinin
(CCK). CCK, besides its other actions, it induces
satiety through its hypothalamic receptors. A
postprandial elevation of CCK is expected for two reasons.
First, since duodenum is in transit (its main site
of secretion), it is able to be stimulated by
nutrients. Second, because small bowel segments that are
not exposed to biliopancreatic juice produce
higher amounts of CCK32,33. Here we also have a
gut segment with nutrients but without
biliopancreatic juice. So, it is reasonable to expect better
CCK secretion. Also, nutrient stimulus in the
duodenum is thought to generate GIP production and a
vagus nerve modulated response that results in an
early stimulus to GLP-1 production in the distal
gut34.
The technique also includes the resection of greater omentum and an enterectomy that
takes out its mesenteric fat. This entails removal
of significant amounts of visceral fat, which is
clearly linked to metabolic syndrome. Visceral fat is
an important source of Plasminogen Activator
Inhibitor 1 (PAI-1)35-37 and
Resistin38-40. Procedures that cause reduction in PAI-1 levels have already been
pointed to for improving metabolic profile and reducing
the cardiovascular risk41,42. Resistin is an inductor
of insulin resistance40.
As visceral fat is insulin resistant, continuous lipolysis generates free fatty acids to
the portal vein, and this is related to hepatic
insulin resistance, diminution in hepatic insulin
clearance and hyperinsulinism43. This provides
additional arguments favoring the removal of visceral
fat. Besides, systemic free fatty acids are related to
a peripheral impairment of insulin
action44; blood lipids and insulin resistance are related to an
inhibition of nitric oxide production (a natural
vasodilator)45 by vascular endothelium, that also links visceral
fat to type II diabetes and hypertension.
As a result of the gastrectomy,
enterectomy and omentectomy, the abdominal pressure
is reduced. This may result in comfort, and
probably less gastroesophageal reflux, a better venous
return and decreased rate of postoperative hernias.
As a significant additional gain, ente-rectomies cause lowering in blood lipids.
Patients presented here and those submitted to
Digestive Adaptation23 presented lowered blood lipids.
This lowering is enhanced by a restriction in
gastric capacity and early satiety.
The proposed procedure, at least
initially, provokes weight loss as efficiently as the
current bariatric procedures. Weight loss ameliorates
the diabetic status, which can be further improved
by visceral fat removal and less production of
Resistin. Better secretion of GLP-1 also helps
improving diabetes. Less food ingestion, less weight,
less cholesterol, less triglycerides, less PAI-1,
normal blood glucose, all together help protect arteries
and the risk of atherothrombotic diseases fall.
There is a possibility that bringing more nutrients to the hindgut may also diminish
the increasing incidence of colon cancer among the obese population of industrialized
countries. Therefore, the adaptation of the Digestive Tract
to modern diet may be a good strategy to help us
face the most incident diseases of modern world.
We think that if we had more physiological procedures to treat obesity, without
prostheses, without obstacles to ingestion of food,
without excluded segments neither unspecific
malabsorption and with a positive neuroendocrine influence
to regulate hunger, satiety and metabolic profile,
we could use this strategy sooner. Adaptive
isolated sleeve gastrectomy or
gastro-omentectomy24, Digestive
Adaptation23 (gastro-omentectomy with enterectomy - Figure 4) and finally
Digestive Adaptation with in-transit Intestinal
Reserve (Figure 2), here proposed, may be a logical line
of procedures to treat obesity, sooner than done nowadays until established severe obesity,
creating a logical progression of procedures to face
the problem in its different stages.
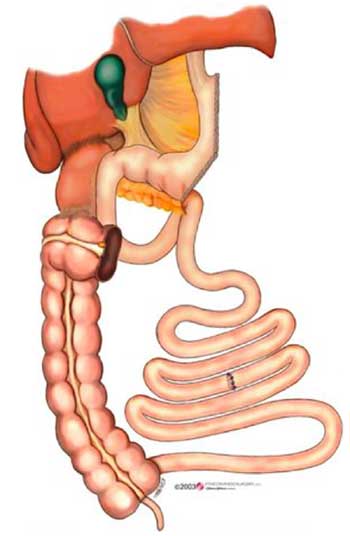 |
| Figure 4 - General aspect of the Digestive Tract after Digestive Adaptation (reference 23). |
The many expected advantages in the field of neuroendocrine response to food ingestion
must be proven also in humans. A significant part of
the evidence for these responses was obtained in
animal models and may not be fully reproduced in humans.
The early results of this new approach are
promising and justify this communication. Longer
follow-up, studies of neuroendocrine peptides production
and a greater number of patients are needed.
Acknowledgements: We thank Ethicon Endo-Surgery,
Inc. for the donation of some of the disposable surgical
equipment used and for the art drawings.
Bibliographic References
1. Castillo J, Fabrega E, Escalante CF, et al.
Liver transplantation in a case of steatohepatitis and
subacute hepatic failure after biliopancreatic diversion for
morbid obesity. Obes Surg 2001;11(5):640-2.
2. Baltasar A, Serra C, Perez N, et al. Clinical
hepatic impairment after duodenal switch. Obes
Surg 2004;14(1):77-83.
3. Beymer, C, Kowdley K, Larson A, et al. Prevalence
and Predictors of Asymptomatic Liver Disease in
Patients Undergoing Gastric Bypass Surgery. Arch
Surg 2003;138(11):1240-1244.
4. Santoro S. Relações entre o comprimento do intestino
e a obesidade. Hipótese: a Síndrome do Intestino
Longo. Einstein 2003;1(1) 63-4. Available in
http://www.einstein.br/biblioteca/
5. Lam NT, Kieffer TJ. The multifaceted potential
of glucagon-like peptide-1 as a therapeutic agent.
Minerva Endocrinol 2002; 27(2):79-93.
6. Egan JM, Meneilly GS, Habener JF, et al.
Glucagon-like Peptide-1 augments insulin-mediated glucose uptake
in the obese state. J Clin Endocrinol Metab 2002;
87 (8):3768-73.
7. Layer P, Holst JJ, Grandt D, et al. Ileal release of
glucagon-like peptide-1 (GLP-1). Association with inhibition
of gastric acid secretion in humans. Dig Dis Sci 1995;40(5):1074-82.
8. Nauck MA; Niedereichholz U; Ettler R; et al.
Glucagon-like peptide 1 inhibition of gastric emptying outweighs
its insulinotropic effects in healthy humans. Am J
Physiol 1997;273(5 Pt 1): E981-8.
9. Schirra J, Wank U, Arnold R, Goke B, Katschinski
M.et al. Effects of glucagon-like peptide-1(7-36) amide
on motility and sensation of the proximal stomach
in humans. Gut 2002;50(3):341-8.
10. Kastin AJ, Akerstrom V, Pan W. Interactions of
glucagon-like peptide-1 (GLP-1) with the blood-brain barrier. J
Mol Neurosci 2002;18(1-2):7-14.
11. Dumont, Y., A. Fournier, S. St-Pierre, et
al. Characterization of neuropeptide Y binding sites in
rat brain membrane preparations using [125I][Leu31,Pro34]peptide YY and [125I]peptide
YY3-36 as selective Y1 and Y2 radioligands. J. Pharmacol.
Exp Ther 1995;272: 673-680.
12. Batterham, R L.; Bloom, S R: The Gut Hormone
Peptide YY Regulates Appetite. Ann NY Acad Sci
2003;994:162-168.
13. Cohen MA, Ellis SM, Le Roux C et al.
Oxyntomodulin Suppresses Appetite and Reduces Food Intake
in Humans. Journal of Clinical Endocrinology & Metabolism 2003;88(10):4696-4701.
14. Ranganath LR, Beety JM, Morgan LM, et al.
Attenuated GLP-1 secretion in obesity: cause or consequence?
Gut 1996;38(6):916-9.
15. Lugari R, Dei Cas A, Ugolotti D, et al. Evidence for
early impairment of glucagon-like peptide 1-induced
insulin secretion in human type 2 (non
insulin-dependent) diabetes. Horm Metab Res 2002;34(3):150-4.
16. Naslund E, Gryback P, Hellstrom PM, et
al. Gastrointestinal hormones and gastric emptying 20
years after jejuno ileal bypass for massive obesity. Int J
Obes Relat Metab Disord 1997, 48:387-92.
17. Bray GA The underlying basis for obesity: relationship
to cancer. J Nutr 2002; 132(11 Suppl):3451S-3455S.
18. Drucker DJ. Glucagon-like peptides: regulators of
cell proliferation, differentiation, and apoptosis.
Mol Endocrinol 2003;17(2):161-71.
19. Dolara P, Caderni G, Salvadori M, et al. Fecal
levels of short-chain fatty acids and bile acids
as determinants of colonic mucosal cell proliferation
in humans. Nutr Cancer 2002;42(2):186-90.
20. Hounnou G, Destrieux C, Desme J, et al.
Anatomical study of the length of the human intestine. Surg
Radiol Anat 2002;24(5):290-4.
21. Aiello L C and Wheeler P. The expensive
tissue hypothesis: The brain and the digestive system in
human and primate evolution. Curr Anthropol 1995;36:199-221.
22. Leonard W R and Robertson M L.
Evolutionary perspectives on human nutrition: The influence of
brain and body size on diet and metabolism. Am J Hum
Biol 1994; 6: 77-88.
23. Santoro S, Velhote MCP, Malzoni CE, et al.
Digestive Adaptation: A new surgical proposal to treat obesity
based in Physiology and Evolution. Einstein
2003;1(2):99-104. Available at http://www.einstein.br/biblioteca/
24. Santoro S, Velhote MC, Mechenas ASG et
al Laparoscopic adaptive gastro-omentectomy as an
early procedure to treat and prevent the progress of
obesity. Rev Bras Videocir 2003;1(3):96-102. Available at
http://www.sobracil.org.br/
25. Muccioli G, Tschop M, Papotti M, et al.
Neuroendocrine and peripheral activities of ghrelin: implications
in metabolism and obesity. Eur J Pharmacol
2002;440(2-3):235-54.
26. Penalva A, Baldelli R, Camina JP, et al. Physiology
and possible pathology of growth hormone secretagogues.
J Pediatr Endocrinol Metab 2001;14 Suppl
5:1207-12; discussion 1261-2.
27. Pinkney J, Williams G. Ghrelin gets hungry.
Lancet 2002;359(9315):1360-1.
28. Vage V, Solhaug JH, Berstad A, et al. Jejunoileal
bypass in the treatment of morbid obesity: a 25-year
follow-up study of 36 patients. Obes Surg 2002;12(3):312-8.
29. Byrne KT. Complications of surgery for obesity. Surg
Clin North Am 2001;81(5):1181-93.
30. Kroyer JM, Talbert WM: Morphological liver changes
in intestinal bypass patients. Am J Surg 1980;139:855-859.
31. Layer P, Holst JJ, Grandt D, et al. Ileal release of
glucagon-like peptide-1 (GLP-1). Association with inhibition
of gastric acid secretion in humans. Dig Dis Sci 1995;40(5):1074-82.
32. Levan VH, Liddle RA, Green GM. Jejunal
bypass stimulation of pancreatic growth and
cholecystokinin secretion in rats: importance of luminal nutrients.
Gut 1987;28 Suppl:25-9.
33. Evrard S, Hoeltzel A, Aprahamian M, et al.
Implication of cholecystokinin in pancreatic adaptation
after biliopancreatic bypass in the rat. Digestion 1994;55(4):208-13.
34. Rocca AS; Brubaker PL. Role of the vagus nerve
in mediating proximal nutrient-induced
glucagon-like peptide-1 secretion. Endocrinology 1999; 140(4): 1687-94.
35. Juhan-Vague I, Alessi MC, Morange PE.
Hypofibrinolysis and increased PAI-1 are linked to atherothrombosis via
insulin resistance and obesity. Ann Med 2000;32 Suppl 1:78-84.
36. Van Hinsbergh VW, Kooistra T, Scheffer MA, et al.
Characterization and fibrinolytic properties of
human omental tissue mesothelial cells. Comparison
with endothelial cells. Blood 1990;75(7):1490-7.
37. Juhan-Vague I, Alessi MC. PAI-1, obesity,
insulin resistance and risk of cardiovascular events.
Thromb Haemost 1997;78(1):656-60.
38. Shojima N, Sakoda H, Ogihara T et al.
Humoral regulation of resistin expression in 3T3-L1 and
mouse adipose cells. Diabetes 2002;51(6):1737-44.
39. McTernan PG, McTernan CL, Chetty R, et al.
Increased resistin gene and protein expression in human
abdominal adipose tissue. J Clin Endocrinol Metab 2002;87(5):2407.
40. McTernan CL, McTernan PG, Harte AL, et al.
Resistin, central obesity, and type 2 diabetes.
Lancet 2002;359(9300):46-7.
41. Carmichael AR, Tate G, King RF, et al. Effects of
the Magenstrasse and Mill operation for obesity on
plasma plasminogen activator inhibitor type 1, tissue
plasminogen activator, fibrinogen and insulin. Pathophysiol
Haemost Thromb 2002;32(1):40-3.
42. Thorne A, Lonnqvist F, Apelman J, et al. A pilot study
of long-term effects of a novel obesity treatment: omentectomy in connection with adjustable
gastric banding. Int J Obes Relat Metab Disord
2002;26(2):193-9.
43. Bergman RN, Van Citters GW, Mittelman SD, et
al. Central role of the adipocyte in the metabolic
syndrome. J Investig Med 2001;49(1):119-126.
44. Storlien LH, Kriketos AD, Calvert GD, et al. Fatty
acids, triglycerides and syndromes of insulin
resistance. Prostaglandins Leukot Essent Fatty Acids 1997;
57(4-5):379-85.
45. Stankevicius E, Kevelaitis E, Vainorius E, et al. Role
of nitric oxide and other endothelium-derived
factors. Medicina 2003;39(4):333-41.
ENDEREÇO PARA CORRESPONDÊNCIA
SÉRGIO SANTORO
Rua São Paulo Antigo, 500/111 SD
São Paulo, SP - Brazil
CEP: 05.684-010
e-mail: ssantoro@ajato.com.br
(1) Hospital Israelita Albert Einstein, São Paulo, Brasil.
(2) Instituto da Criança, Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, Brasil.
(3) Hospital da Policia Militar do Estado de São Paulo, Brasil.