|
|
Official Journal of the
|
ISSN: 1983-991X
|
|
| Case Report « PDF file » |
|
Transumbilical Laparoscopic Bilateral Nephrectomy
Aníbal Wood Branco1; William Kondo2; Luciano Carneiro Stunitz3; Alcides José Branco Filho4
1 Urologist - Hospital da Cruz Vermelha. 2 General Surgeon and Gynecologist - Hospital da Cruz Vermelha. 3 Urologist - Hospital da Cruz Vermelha. 4 General Surgeon - Hospital da Cruz Vermelha.
ABSTRACT
Introduction: Traditionally, the laparoscopic surgeries use several trocars (three to six) introduced by transperitoneal
or retroperitoneal access, depending on the type and the complexity of the procedure. Thus, the optimum triangulation
is reached. That triangulation has been considered an essential pre requisite for the complex surgical procedures
that need precise dissections and suturing techniques. Lately some authors have attempted to reduce even more
the morbidity of the laparoscopy carrying mini-laparoscopy surgeries through natural orifices and transumbilical
access. The intention of this article is to describe a case of bilateral nephrectomy for instrumental laparoscopic
transumbilical access using of conventional laparoscopic surgery. Case report: 60-year-old female patient, who underwent
renal transplant with graft in the right iliac fossa, was directed to our group by the nephrology service due to repetition
urinary tract infection and bilateral renal atrophy. An evaluation of the possibility of proceeding bilateral laparoscopic
nephrectomy was carried out, and based on this pre-surgery evaluation, the indicated procedure was through transumbilical
access. After the confection of the pneumoperitoneum, three trocars had been located within the periumbilical region and
the surgery was successfully carried through without the use of any articulated laparoscopic instrument. The operative
time was 100 minutes, with an estimated 100 ml blood loss. The patient got discharged from the hospital on the second
day of the postoperative period. Conclusion: The accomplishment of bilateral nephrectomy through transumbilical
laparoscopic access is feasible and this access can be considered an alternative to the traditional laparoscopy, even when
special articulated laparoscopic instruments are not available.
Key words: Transumbilical surgery, Single port, Single incision, Laparoscopy, E NOTES.
Bras. J. Video-Sur, 2009, v. 2, n. 4: 033-041
| Accepted after revision: February, 11, 2009. |
INTRODUCTION
n the past few years, the minimum invasive surgery
dramatically changed the surgical conception.
Some complex procedures performed exclusively
through open surgery today are currently approached
through laparoscopy in excellence centers. The
advantages of the minimum invasive overture include
little postoperative pain, lesser in-hospital time,
faster recovery and superior esthetic
effect1.
Traditionally, the laparoscopic surgeries use several trocars (three to six) introduced
through transperitoneal or retroperitoneal
access2, depending on the type and the complexity of
procedimento3. In this, the optimum triangulation, which has
been considered an essential pre requisite for the
complex surgical procedures that need precise dissections
and suturing techniques, is reached4.
More recently, researches have been directed towards the development of strategies to reduce
the morbidity in these surgeries even more, and to
improve the esthetic results4. This includes the reduction
of the size of the portals
(mini-laparoscopy)5, the use of the surgery through natural orifices (NOTES,
natural orifice translumenal endoscopic
surgery)6-11 and of the access
transumbilical2-4-11-25. In the latter, it
is assumed that the umbilicus is an embryonic
natural orifice (e) that can be used as a point of access to
the abdominal cavity for surgical procedures, since it
is considered a scar. Gill et al12 had proposed the term
E NOTES (embryonic natural orifice
transumbilical endoscopic surgery) for this via. Other terms
which have already been used to describe this technique
are TUES (transumbilical endoscopic surgery),
NOTES (natural orifices transumbilical
surgery), and also single port, single
access, single incision or keyhole
surgery, all based on the principle of an only abdominal incision inserting articulated
laparoscopic instruments15,26,27.
The possibility of using the transumbilical access to carry through surgical procedures
was initially demonstrated in a swine experimental
model by PARK et al28 and confirmed by various authors
in human beings2-4,12-25. Many devices have
been developed to allow the introduction of some laparoscopic instruments through a single incision
on the skin2 (R port2,12, Uni X Single Port
Access Laparoscopic System3,
Gelport20 and SITRACC29), but they are still onerous, which might restrict
their use in developing countries. RAMAN et
al15 were the first ones to report about nephrectomy through
a single umbilical incision using 3 conventional
trocars located separately as well as special
articulated instruments, as an alternative to the use of the
single port equipment. Since many services do not
make use of articulated instrument, some authors
have described the accomplishment of successful transumbilicais surgeries using trocars
and conventional instruments of
laparoscopy14.
In this article, we describe a case of
bilateral nephrectomy using the transumbilical access
and conventional instruments of laparoscopic surgery.
CASE REPORT
60-year-old female patient, who underwent renal transplant with graft in the right iliac fossa,
was directed to our group by the service of
nephrology due to repetition urinary tract infection and
bilateral renal atrophy to have evaluated the possibility
of proceeding of bilateral laparoscopic nephrectomy.
After the pre-operative evaluation and confirmation of the indication of the procedure,
we considered the accomplishment of bilateral laparoscopic nephrectomy through
transumbilical access.
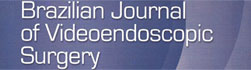
Under general anesthesia, the patient was initially positioned on left lateral decubitus to have
the right nephrectomy (Figure. 1A). The Veress
needle was located through the umbilicus (Figure.
1B), allowing the insufflation of carbon dioxide in the
abdominal cavity. The intra-abdominal pressure was mantained between 12 and 14mmHg. A 10mm
trocar was located in the periumbilical region for a
30-degree optic, followed by the positioning of 2
additional periumbilical trocars (5mm and 10mm ones)
(Figure 1C). This way the surgeon worked using two
portals with the instruments in parallel (Figure 1D).
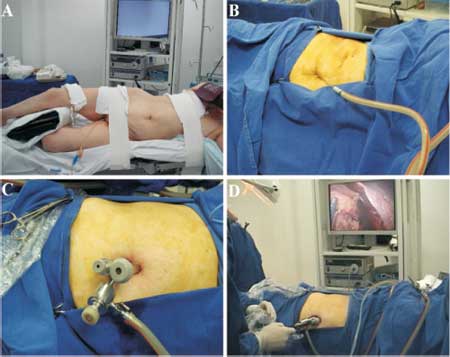 |
Figure 1 - (A) Patient placed on left lateral decubitus position. (B) Creation of pneumoperitoneum with a transumbilical Veress needle. (C) Placement of the transumbilical trocars. (D) External manipulation of the forceps. |
The surgery steps had been the same ones carried through in the conventional
laparoscopic surgery. Summing up, the ascending colon
was mobilized medially after the opening of the
right parietocolic leak on Toldt white line using
electric-cauterization. The kidney was gradually released
from its lateral, superior, inferior and posterior
adherences. The renal hilo was accessed and the main renal
vases were dissected and isolated. After binding with LT
300 titanium and 10mm Hem o lok clips (Weck
Closure Systems, Research Triangle Park, NC), the
renal vessels were divided (Figures 2A, 2B and 2C).
The ureter was dissected, bonded with a LT 300
titanium clip (Figure 2D), and later sectioned.
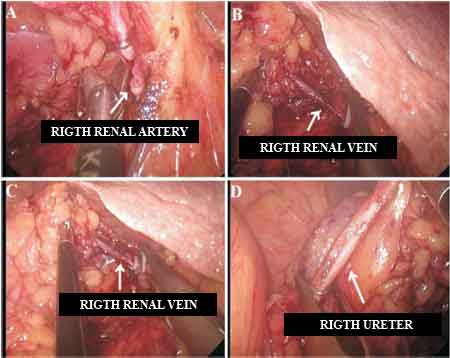 |
Figure 2 - (A) Ligature and sectioning of the right renal artery. (B and C) Ligature of the right renal vein with Hem-o-lok clips. (D) Ligature the right ureter |
The patient was placed on right lateral decubitus position and the same procedure
previously described was carried through for the left
nephrectomy (Figures 3A, 3B, 3C and 3D).
 |
Figure 3 - (A) Ligature of the left renal artery with Hem-o-lok clips. (B and C) Ligature of the left renal veins with Hem-o-lok clips. (D) Ligature of the left ureter |
The kidneys were placed in a bag and kept with clamps (Figure 4A). Trocars were removed
and the 3 periumbilical incisions on the skin were
joined. The opening of the abdominal aponeurosis
was enlarged and the bag was removed of its cavity
(Figure 4B). The closing of the aponeurosis and the
skin was carried through with polyglactin 910
(Vycril®) and 4/0 mono nylon (Figure 4C), respectively.
The operative time was 100 minutes, with an estimated 100 ml blood loss. The
post-operative analgesia was carried through with dipirone (1
gram intra vein each 6 hours) and cetoprofen (100mg
intra vein each 12 hours). The patient got discharged
from the hospital on the second day of the
postoperative period.
The anatomic-pathological report accused renal atrophy and chronic pyelonephritis (Figure 4D).
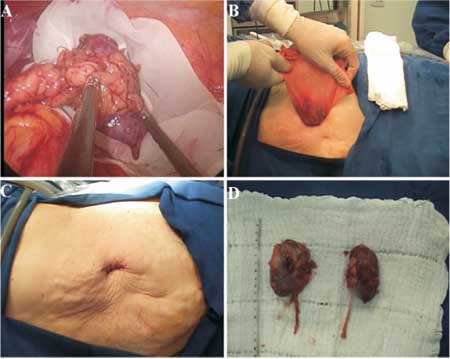 |
Figure 4 - (A) Placing the kidneys in an extraction bag. (B) Taking kidneys out of the abdominal cavity. (C) Final aspect of the abdomen. (D) Surgical specimens |
DISCUSSION
One of the basic pre-requisites for the advanced laparoscopic surgery is the
correct positioning of the portals in such a way that there is
a minimum distance between them, allowing a wide
range of movements and also preventing the collision
of the instruments. This still enables the
triangulation between the instruments and the optics, which
is essential in carrying through the surgical
dissection and intracorporeal suturing.
The concept of transumbilical surgery includes the positioning of a single trocar with various
working channels in the umbilical region or three
conventional adjacent periumbilical trocars, so that the optics
and the instruments are disposed in parallel within the
abdominal cavity. This parallel positioning makes
the surgical procedure more difficult since there is
internal and external collision of the instruments during
their manipulation. The development of optics and
5mm flexible instruments partially helped overcome
this technical difficulty, even thought the instruments
are introduced adjacent and parallel to one another
through a single portal.
Some urologic procedures through transumbilical access have been described
with encouraging results (Table 1). Special trocars
with some articulated working channels
(R-port2,12, Uni X Single Port Access Laparoscopic
System3, Gelport20 and
SITRACC29) and laparoscopic instruments
have been developed not only to make possible but also
to facilitate the laparoscopic surgery using only
one incision; however, they are still expensive
and impracticable for many surgery groups in
developing countries.
 |
The advantages of the transumbilical surgery are: (1) the technique is similar to the
traditional laparoscopy27, (2) the orientation is easily
controlled by the assistant, thus, the surgeon can get
better images, similarly to the convencional
laparoscopy26, (3) the technique minimizes the morbidity related
to the skin incisions (muscular pain and spasms in
the incision, prevents lesions of epigastric vessels),
(4) incision can be hidden inside the umbilicus
(better esthetic effect)3,23,30, (5) the method allows that
the surgeon converts the procedure to a
conventional laparoscopic surgery at any time, if necessary,
adding one or more conventional laparoscopic
trocars3,25, (6) the procedure is simpler and safer than the
NOTES techniques26.
The disadvantages are: (1) the parallel positioning and close to the instruments enough
tending to result in the collision between the optics and
the instruments2,12,30, requiring a significant
coordination between surgeon and
camera3,30, (2) dissection through a single trocar is more difficult than that
in the conventional laparoscopy with various
trocars2,30 due to the lack of triangulation of the instruments,
and (3) the costs of the single ports and the
articulated instruments.
In this article we report a case of bilateral transumbilical laparoscopic nephrectomy
using instruments of conventional laparoscopic surgery
and 3 adjacent periumbilicais punctures. The
surgery exposure was adequate and the steps for
the conventional laparoscopy could be reproduced
within the transumbilical technique. No great difficulty
was observed during the procedure. As all the trocars
were placed in the periumbilical region, at the end of
the surgery incisions were easily joined in order to
remove the surgical specimen.
We found the same problems previously mentioned by RAMAN et
al15 in relation to the intra and extra abdominal collision of the
instruments; however, we could prove that it is feasible to
carry through the same procedure without
articulated laparoscopic instruments. The coordination
between surgeon and assistant is essential to minimize
the internal and external collisions of the instrument.
The renal vessels ligation were easily performed
with 10mm Hem o lok and LT 300 titanium clips,
sparing the use of vascular endo staplers.
We believe that the transumbilical access is a potential alternative for the traditional laparoscopy,
with a better esthetic effect since there is only one
umbilical incision and a reduction of the complications
related to incisions on the skin. The learning curve exists,
but it is significantly lower than that in NOTES. We
expect prospective and random studies to really evaluate
the effectiveness, the indications and the benefits of
the transumbilical surgery compared to the
traditional laparoscopy.
REFERENCES
1. Hemal AK, Talwar M, Wadhwa SN, Gupta
NP. Retroperitoneoscopic nephrectomy for benign
diseases of the kidney: prospective nonrandomized
comparison with open surgical nephrectomy. J Endourol 1999;
13: 425-31.
2. Desai MM, Rao PP, Aron M, Pascal-Haber G, Desai
MR, Mishra S, et al. Scarless single port
transumbilical nephrectomy and pyeloplasty: first clinical report. BJU
Int 2008; 101: 83-8.
3. Kaouk JH, Haber GP, Goel RK, Desai MM, Aron
M, Rackley RR, et al. Single-port laparoscopic surgery
in urology: initial experience. Urology 2008; 71: 3-6.
4. Desai MM, Stein R, Rao P, Canes D, Aron M, Rao PP, et
al. Embryonic natural orifice transumbilical endoscopic
surgery (E-NOTES) for advanced reconstruction: initial
experience. Urology 2009; 73: 182-7.
5. Soble JJ, Gill IS. Needlescopic urology: incorporating
2-mm instruments in laparoscopic surgery. Urology 1998; 52: 187-94.
6. Gettman MT, Lotan Y, Napper CA, Cadeddu
JA. Transvaginal laparoscopic nephrectomy: development
and feasibility in the porcine model. Urology 2002; 59: 446-50.
7. Marescaux J, Dallemagne B, Perretta S, Wattiez A, Mutter
D, Coumaros D. Surgery without scars: report of
transluminal cholecystectomy in a human being. Arch Surg 2007; 142: 823-6.
8. Branco AW, Branco Filho AJ, Kondo W, Noda RW,
Kawahara N, Camargo AA, et al. Hybrid transvaginal
nephrectomy. Eur Urol 2008; 53: 1290-4.
9. Branco Filho AJ, Noda RW, Kondo W, Kawahara N,
Rangel M, Branco AW. Initial experience with hybrid
transvaginal cholecystectomy. Gastrointest Endosc 2007; 66: 1245-8.
10. Clayman RV, Box GN, Abraham JB, Lee HJ, Deane
LA, Sargent ER, et al. Rapid communication: transvaginal
single-port NOTES nephrectomy: initial laboratory experience.
J Endourol 2007; 21: 640-4.
11. Kondo W, Noda RW, Branco AW, Rangel M, Filho
AJ. Transvaginal endoscopic tubal sterilization: a case report.
J Laparoendosc Adv Surg Tech A 2009. (A ser publicado).
12. Gill IS, Canes D, Aron M, Haber GP, Goldfarb DA,
Flechner S, et al. Single port transumbilical (E-NOTES)
donor nephrectomy. J Urol 2008; 180: 637-41.
13. Rané A, Rao P, Rao P. Single-port-access nephrectomy
and other laparoscopic urologic procedures using a
novel laparoscopic port (R-port). Urology 2008; 72: 260-3.
14. Branco AW, Branco Filho AJ, Noda RW, George
MA, Camargo AHLA, Kondo W. New minimally invasive
surgical approaches: transvaginal and transumbilical. Bras J
Video-Sur 2008; 1: 29-36.
15. Raman JD, Bensalah K, Bagrodia A, Stern JM, Cadeddu
JA. Laboratory and clinical development of single keyhole
umbilical nephrectomy. Urology 2007; 70: 1039-42.
16. Kaouk JH, Palmer JS. Single-port laparoscopic
surgery: initial experience in children for varicocelectomy. BJU
Int 2008; 102: 97-9.
17. Kaouk JH, Goel RK, Haber GP, Crouzet S, Desai MM,
Gill IS. Single-port laparoscopic radical prostatectomy.
Urology 2008; 72: 1190-3.
18. Kaouk JH, Goel RK, Haber GP, Crouzet S, Stein RJ.
Robotic single-port transumbilical surgery in humans: initial
report. BJU Int 2009; 103 :366-9.
19. Walz MK, Alesina PF. Single access
retroperitoneoscopic adrenalectomy (SARA)-one step beyond in
endocrine surgery. Langenbecks Arch Surg 2008. (A ser
publicado).
20. Ponsky LE, Cherullo EE, Sawyer M, Hartke D. Single
access site laparoscopic radical nephrectomy: initial
clinical experience. J Endourol 2008; 22: 663-6.
21. Castellucci SA, Curcillo PG, Ginsberg PC, Saba SC, Jaffe
JS, Harmon JD. Single port access adrenalectomy. J
Endourol 2008; 22: 1573-6.
22. Goel RK, Kaouk JH. Single port access renal
cryoablation (SPARC): a new approach. Eur Urol 2008; 53: 1204-9.
23. Raman JD, Bagrodia A, Cadeddu JA. Single-Incision,
Umbilical Laparoscopic versus Conventional
Laparoscopic Nephrectomy: A Comparison of Perioperative
Outcomes and Short-Term Measures of Convalescence. Eur Urol
2008. (A ser publicado).
24. Desai MM, Aron M, Canes D, Fareed K, Carmona O,
Haber GP, et al. Single-port transvesical simple
prostatectomy: initial clinical report. Urology 2008; 72: 960-5.
25. Aron M, Canes D, Desai MM, Haber GP, Kaouk JH,
Gill IS. Transumbilical single-port laparoscopic
partial nephrectomy. BJU Int 2009; 103: 516-21.
26. Zhu JF. Scarless endoscopic surgery: NOTES or
TUES. Surg Endosc 2007; 21: 1898-9.
27. Gettman MT, Box G, Averch T, Cadeddu JA, Cherullo
E, Clayman RV, et al. Consensus statement on natural
orifice transluminal endoscopic surgery and
single-incision laparoscopic surgery: heralding a new era in urology?
Eur Urol 2008; 53: 1117-20.
28. Park S, Bergs RA, Eberhart R, Baker L, Fernandez R,
Cadeddu JA. Trocar-less instrumentation for laparoscopy:
magnetic positioning of intra-abdominal camera and retractor. Ann
Surg 2007; 245: 379-84.
29. Martins MVDC, Skinovsky J, Coelho DE, Torres
MF. SITRACC Single trocar access: a new device for a
new surgical approach. Bras J Video-Sur 2008; 1: 61-3.
30. Canes D, Desai MM, Aron M, Haber GP, Goel RK,
Stein RJ, et al. Transumbilical single-port surgery: evolution
and current status. Eur Urol 2008; 54: 1020-9.
Correspondence address:
Dr. William Kondo
Avenida Getulio Vargas, 3163 / ap 21
Curitiba - PR
CEP 80240-041
Phone: (41) 9222-1065