|
|
Official Journal of the
|
ISSN: 1983-991X
|
|
| Original Article « PDF file » |
|
Videolaparoscopic Cholecystectomy with Two Ports: Preliminary Report
Elton Francisco Nunes Batista1, Carlos Alberto de Castro Fagundes2, Cristiano de Souza Pinto3 , Gustavo Adolfo Pavan Batista4
1. Member of Sobracil. TCBC. Adjunct Professor of the Departament of Clinical Surgery Center of Health Science of the Federal University of Espírito Santo Discipline of Operative Technique and Experimental Surgery; 2. General Surgeon and Proctologist Hospital Dr. Dório Silva e Coordinator of the ATLS Program of Espírito Santo; 1, 2 e 3. CIAS Surgeons Centro Integrado de Atenção a Saúde (Unimed Vitória); 4. Physician.
ABSTRACT
With unquestionable benefits the laparoscopic surgery begins a phase of reduction of accesses. After
minilaparoscopy, now emerges the unique umbilical access and NOTES. These novelties are restricted to some Centers due to the
high cost, difficulty to sterilize instruments, and necessity of new and intensive training. As these procedures are still in
an experimental phase they are not surely for all professionals. Following the same line of study to reduce accesses, we
are developing laparoscopic cholecystectomy with only two trocars (umbical and subxiphoid) in which the surgery is
almost scarless. This method is extremely simple and available to surgeons in any institution and it does not require
another type of training besides the one that has been already obtained for laparoscopy. Moreover the same optical and
surgical instruments are used, and at first it should only be performed in selected cases. The exposition of the gallbladder
is simple and it can be accomplished using alternatives that are available in any surgical center. We were able to
perform the proposed procedure with the same safety used with multiple ports access. With only six patients who were
selected following the criterion of low weight for the initial selection of patients. The last patient did not follow our initial criterion
of selection as the patient was a bit overweight. The operative time was between 30 and 50 minutes, basically the
same mean time spend with multiple port accesses.
Key words: cholecystectomy, laparoscopic surgery, surgical technique and method, minimally invasive surgery.
Bras. J. Video-Sur, 2009, v. 2, n. 4: 027-032
| Accepted after revision: January, 19, 2009. |
INTRODUCTION
ideoendoscopic surgery has brought
unquestionable benefits to patients as well as
to surgeons. Benefits to patients because it offers
with a small access the same possible operative
techniques of the conventional surgery with
considerable reduction of trauma and less organic
repercussion mainly pain and infection. Avoiding large incisions
have also brought cosmetics gain, reduced complication
of the wall, better metabolic response to the surgical
trauma and earlier return to work. To the surgeon
the benefits elapse from less work with the patient due
to reduce operative time, low incidence of
postoperative intercurrences, in spite of the possibility of earlier
hospital discharge, which will give the surgeon more
time for other activities.
As surgeons become more skilled and expert their horizons are enlarged and the innovations
appear. Every day new facilitator methods, access
alternatives and forms of approaches that have never
been imagined appear seeking to offer something
new whose benefits are debatable. The innovation of
the laparoscopic technique established in substitution
to the conventional surgery was only satisfactory
during the necessary time to break the barriers of contraindications and of restrictions of indication
for certain diseases. Nowadays, the indications
have multiplied new approaches alternatives are
being introduced and discussed worldwide and the restrictions almost disappeared. When
everything seemed to be already consolidated with time
the surgeon started to worry again about incisions
and forms of approaches and these aspects are on
the agenda in every medical event. Once again the
surgeon searching for artifices to improve what it has
already been demonstrated to be very good.
So, to reduce incisions emerges minilaparoscopy that reduce the diameter of
the instruments, the needlescopic cholecystectomy
with 2mm instruments, the single port access that
enables simultaneous passage of several instruments
and NOTES, basically still experimental and that technically seeks to avoid abdominal
incision. However, such innovations are restricted to
certain institutions due to costs, instruments fragility,
difficulty to sterilize instruments, and necessity of new
and intensive training. Thus, it can be inferred that
these recent novelties are available to few professionals.
To be available to a greater number of
professionals, we are now developing the
laparoscopic cholecystectomy technique with only two trocars
(umbilical and subxiphoid) aided with the exposition of
the gallbladder by external traction without incision.
The surgical procedure with this method is almost
scarless as well as extremely simple and accessible to
any surgeon in addition this procedure does not
demand training besides the one that has already been
obtained for laparoscopy and the instruments used are the
same habitual, either the optical or the work
instruments. The exposition of the gallbladder is simple
using alternatives that are available in any surgical
center and the technique does not differ in anything
from what it is already known and habitually practiced.
At first it should be used only in selected cases.
SURGICAL TECHNIQUE AND METHODS
The patient is positioned in dorsal decubitus position, and fastened at the basis of the
thigh to allow safe movement of the operative table during
surgery. The operative fields are placed as usual. The
umbilical port is performed using the open method to
insert an 11mm trocar and pneumoperitoneum is created
with an intrabdominal pressure limit of 12 mmHg. A
30 degree 10mm telescope is inserted to inspect the
abdominal cavity and a second 6mm subxiphoid
trocar is inserted under laparoscopic vision. All
instruments necessary to the surgery are going to be used
through this port as well as external ligatures as clips are
not used. (Figure 1)
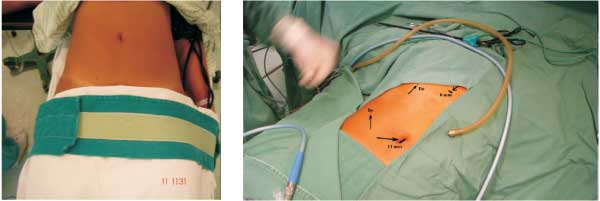 |
Figure 1 - a) Position on the table; b) Preparation of the operative field and references of the ports. |
The following alternative methods were used to expose the gallbladder pedicle:
1) First a 2-0 thread with a 3 cm needle previously curved as a hook is inserted into the
serosa at the fundus of the gallbladder. The next step is
to insert a 40/12 needle in the first intercostal space
above the right costal margin with a 0-looped nylon
thread from where the extremity of the 2-0 thread will
be retrieved. This port elevates the right lobe of the
liver by the traction of the gallbladder fundus
substituting the right flank forceps. The previous surgical
maneuver is repeated and the other extremity of the thread
is retrieved at the level of the right flank at the
umbilicus. The hooked need is fixed in the infundibulo
substituting the subcostal forceps. The extremities of both
threads are maintained with clamping close to the skin.
(Figures 2 and 3).
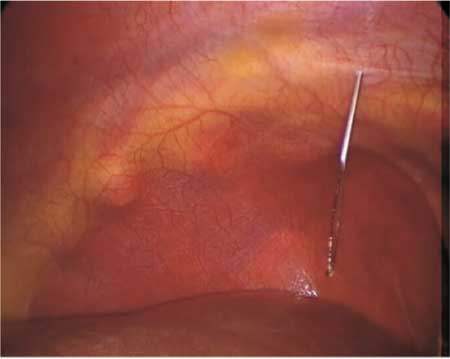 |
Figure 2 - Insertion of 40/12 needle with a thread loop to retrieve
the 2-0 nylon thread. |
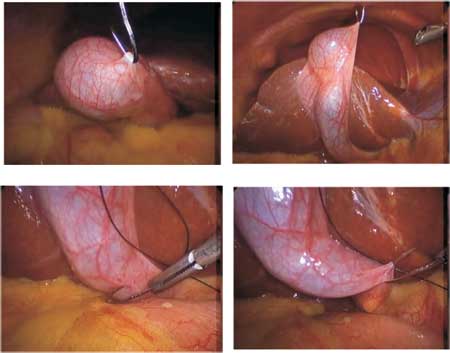 |
Figure 3 - a) Repair of fundus; b) Traction of the fundus and elevation of the hepatic lobe; c e d) Repair of the infundibulo. |
2) the other alternative is the introduction of a 2-0 thread directly to the wall, in the sites
mentioned above. After the visualization of the needle, it
is retrieved and exteriorized by the subxiphoid port
to gain the shape of a hook and then the needle
once again is inserted in the abdominal cavity repair
the fundus and the infundibulo, respectively. This
method is much simpler and quick; (Figure 4)
 |
Figure 4 - a) Direct passage of the needle through the intercostal space; b) Passage of the needle through the flank. |
Whichever method is adopted to expose the gallbladder pedicle, the surgical procedure
is traditionally performed using dissecting
forceps, scissors, hook and external knots pusher. The
thread of needle that pulls the infundibulo is
manipulated externally by the surgeon and the needle may
be repositioned at any moment of the surgery in
different parts of the gallbladder, while it has been
removed from the liver bed (Figure 5).
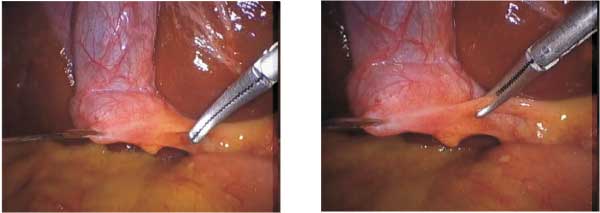 |
Figure 5 - a) Gallbladder tractioned by threads; b) Beginning of the dissection. Traction of the gallbladder fundus and infundibulo allows its pedicle to be well exposed which considerably facilitates the sequence of the dissection and hemostasis. |
Traction of the gallbladder fundus and infundibulo allows its pedicle to be well exposed
which considerably facilitates the sequence of the
dissection and hemostasis (Figure 6).
 |
Figure 6 - a) External aspect of the trocars and traction threads; b) Final result: two small incisions. |
Our case series is still very little expressive because the method was only adopted in 6 patients. The criterion used for the initial selection of patients was low weight and in five patients the procedure was easily performed with the same safety used with multiple port access. The last patient was a bit overweight; therefore, we did not follow our initial criterion, there was not observed as well any technical difficulty. The operative time was between 30 and 50 minutes, basically the same mean time spend with multiple port accesses.
DISCUSSION
It is a fact that the benefits of
videoendoscopic surgery are unquestionable. With small ports, it
offers the same technical possibilities of the
conventional surgery, minimizing the trauma of the wall and
with less organic repercussion. Avoiding big
incisions brought cosmetics gain, the complications of the
abdominal wall almost disappear and it still allows
an early return to work for the patient. Even with all
these advantages the surgeon still search for ways
to improve what it has been shown to be already
very good. In order to reduce even more the incisions,
it has emerged minilaparoscopy3 that uses
instruments with small diameter (3mm),
needlescopic cholecystectomy with 2mm instruments, the single
port access5 which enable the passage of
several instruments and NOTES4 that is still an
experimental procedure that technically tries to avoid
abdominal incisions. However, such novelties due to the
elevated cost, the difficulty to sterilize instruments and
the necessity of new and intensive are restricted to
some institutions. So, it is evident that these innovations
will only be available for few professionals.
The classical laparoscopic cholecystectomy uses the four ports technique. Some surgeons
use only three trocars. In our routine, we have
already been using in the majority of the
cholecystectomies only three trocars(umbilical, subxiphoid and
right subcostal) sometimes with the help of a
small traction of the gallbladder fundus to elevate the
lobe of the liver. Nowadays, we are developing laparoscopic cholecystectomy with only two
trocars with external traction of the threads. It was
not observed any major technical difficult regarding
the sources of exposition. The difficulties have
been the same when compared to the multiple
accesses previously adopted. Our experience is with only
six surgeries with no complications and the fact
that not every patient was thin.
The external control of the thread has already been
suggested to expose the pedicle in other surgeries.
Batista1 and cols have demonstrated
the versatility of the external control of threads and
the simplicity that this resource offers to
splenectomy which was considered a surgery with a high
degree of difficulty. For cholecystectomy, the
method presented is initially suggested for selected cases,
and certainly it can be used by the majority of the
surgeons that intend to reduce the number of incisions in
this surgical procedure. The cholecystectomy
performed with only two trocars is extremely simple and
available to surgeons of any institution because it does
not requires another type of training besides the one
that has been already acquired for
laparoscopy2. The resources used for this technique are also simple
and there has neither modification nor adaptation to
the instruments habitually used. The exposition of
the gallbladder may be done with simple alternative
using the resources that are available in any surgical
center. Besides, the technique does not differ from what
is already known and habitually practiced in cholecystectomies with three or four trocars.
CONCLUSION
Laparoscopic cholecystectomy with only two ports accesses with incisions of 1.2cm in the umbilicus and 0.6cm subxiphoid easily allowed the surgery to be performed in the first six patients that the procedure was suggested. The criterion to select only thin patients (60 to 70kg of weight) was not observed in the sixth patient who was considerably overweight (over 85 kg) for the proposed method. There was not any complication and the duration of the operative time varied from 30 minutes to 50 minutes (mean time 44 minutes). Even so, we consider fundamental an adequate selection of patients and in case of difficulty we suggest the addition of more trocars.
REFERENCES
1. Batista, E.F.N; Del Caro, S.R.; Ruschi, M.C.N.;
Ferreira, M.A.B.; Ruschi Filho, A.A. & Batista,
G.A.P. Esplenectomia laparoscópica Contribuição tática pelo
uso de alça externa de fio de nylon para exposição do
pedículo. Revista Brasileira de Videocirurgia, v.4 n.2, Abr/Jun
2006, p. 70-4.
2. Batista, E.F.N.; Do Carmo, J.W.C. Silva, A.A.; Biccas, Jr.,
L. & Carneiro, J.L.A.; Lemos, A.G. & Lemos,
A.S. Colecistectomia laparoscópica adestramento em
modelo experimental vivo. Rev. Col. Bras. Cir., Vol. XX (6):
301-4, Nov., 19 93.
3. Carvalho, G.L.; Silva, F.W.; Cavalcanti, C.H.; Albuquerque,
P.P.C.; Araújo, D.G.; Vilaça, T.G. & Lacerda,
C.M. Colecistectomia minilaparoscópica sem utilização
de endoclipes: técnica e resultados em 719 casos.
Revista Brasileira de Videocirurgia, v. 5 n. 1, Jan/Mar 2007, p.
5-11.
4. Souza, L.H.; Souza Filho, L.H.; Souza, V.M.;
Souza, J.A.G.; Tamura, S. & Chalela, Jr., D. Colecistectomia endoscópica: proposta de nova
técnica totalmente transluminal por orifícios naturais.
Resultado inicial de estudo experimental em suínos. Revista
Brasileira de Videocirurgia, v. 5 n. 2, Abr/Jun 2007, p.
90-102.
5. Martins, M.V.D.C; Skinovsky, J; Coelho, D.C. &
Torres, M.F. Sitracc Single trocar Access: a new device for a
new surgical approach. Bras. J. Video-Sur, v. 1 n. 2,
Apr/Jun 2008, p. 61-3.
Correspondence address:
Elton Francisco Nunes Batista
Rua Dr. Antônio Honório, 75 Bento Ferreira
29050-770 VITÓRIA ES
Email: eltonmed@yahoo.com.br
Home: www.elton.med.br