|
|
Official Journal of the
|
ISSN: 1983-991X
|
|
| Case Report « PDF file » |
|
Laparoscopic Transperitoneal Nephropexy without Using Intracorporeal Knot
Lessandro Curcio; Antonio Claudio Cunha; Juan Renteria; Fabrizio Costa; Rodolfo Roca; Geraldo Di Biase
1 Hospital Geral de Ipanema - Urology Service - Laparoscopy and Minimally Invasive Surgery Sector.
ABSTRACT
Introducion: The downward displacement of the kidney (nephroptosis) when in orthostatic position may lead to incapacitating symptoms especially pain (which is believed to be due to temporary ischemia of the kidney); requiring surgical fixation of this organ to peritoneal muscles and ligaments. Laparoscopic is very efficient in these cases, either transretroperioneal or retroperitoneal bringing benefits to patients. We reported a successful case in which we performed the renal fixation without using intracorporeal knot. Report: A 65-year-old woman with pain in the right lumbar region. Excretory urography revealed a downward displacement of the right kidney when the position is changed from supine to orthostatic, as well as ipsilateral kink in the ureter. Transperitoneal nephropexy was performed with four trocars and suture was performed with a monofilamentary non-absorbable thread with the extremities tied to a polymer clip(Hem-o-lok® - Pilling Weck) to fix the kidney. The operative time was 240 minutes with very little blood loss and after 3 days of hospital stay the patient was discharged. It was observed pain and paresthesia in right inferior member that improved with the use of gabepentin for a month. Conclusion: Laparoscopic nephropexy has encouraging outcomes (80-100%), which contrasts a little with the open technique, in spite of the fact that there is no prospective and randomized study comparing the two techniques. The kidney fixation with polymer clips (similar to what is used in the partial laparoscopic nephrectomy) may be a good alternative to avoid complications and failures in the treatment of the renal ptosis.
Key words: laparoscopy, nephroptosis, nephropexy.
Bras. J. Video-Sur, 2008, v. 1, n. 4: 171-174
| Accepted after revision: August, 14, 2008. |
INTRODUCTION
ephroptosis was first described in Germany by
Hahn and the first textbooks have already defined it as a downward displacement of the
kidney in a cranio _caudal direction by more than 5cm or
by a downward of two vertebral bodies(by
urography)1. In the 70 and 80 decades, many open
nephropexy surgeries were performed with a 68.6% success
rate2, so the procedure was not considered reliable until
the advent of laparoscopic urology.
The transperitoneal approach has as it
main advantage, a greater workspace and the retroperitoneal approach may be used, with a
similar successful rate, depending on the experience of
the surgeon with the technique. As well as the choice
of the approach, the use of mesh or not depends on
the urologist self-confidence on the suture performed.
We describe our technique of laparoscopic nephropexy with the use of the extremities
of prolypropylene threads tied with a polymer clip
that after inserting them in the muscle and in the infrahepatic peritoneum a second clip is used in
the other extremity to tighten it, this technique is used
to save time during the laparoscopic partial nephrectomy.
CASE REPORT AND TECHNIQUE
A 65-year-old patient with controlled hypertension without previous history of
trauma, lithiasis and weight loss complained about severe
pain in the right lumbar, with no association with
hydric ingestion and which got worse when she stood up
for a long period doing an activity (such as sweep
the floor). Because of this pain she went several times
to the emergency room of different hospitals.
Echography depicted a slight dilation of the right kidney and
an abnormal renal mobility when the ultrasound
probe was being inserted in the right flank.
Excretory urography revealed that the kidney descended
more than 5 cm as well as two vertebral bodies of the
right kidney when the position is changed from supine
(Figure 1) to orthostatic (Figure 2). Based on the diagnosis of nephroptosis laparoscopic
nephropexy was indicated.
 |
Figure 1 - Excretory urography in supine position showing
the initial position of the right kidney. |
 |
Figure 2 - Excretory urography in upright position showing
sever displacement of the organ. |
The patient was placed in the left half-lateral decubitus position with pads to relieve the
pressure over some areas. Two 10mm trocars and two
5mm trocars were used, one at the umbilicus where it
was inserted a 30o optical the other 10mm was inserted
12 cm from this one in the middle line. One 5 mm
trocar was inserted at the midline between the
right anterosuperior iliac spine and the umbilicus and at
last a 5 mm trocar is inserted two fingers below the
furcula to move the liver. The right colon and duodenum
were repelled to the midline and the kidney with its
perirenal fat was identified. The fat was removed from the
lateral part (Figure 3) until the capsule could be
seen, remaining just slightly close to the hilum. At
this moment, the patient was placed in Tredlemburg
position in order to be investigated the correct position of
the kidney that was going to be fixed. Three 2.0 polypropylene threads were inserted into the
lateral border of the kidney and they were temporarily
fixed into the lateral abdominal wall. Another suture of
the same thread was passed through the upper pole
of the kidney and afterwards into the infrahepatic peritoneum which was tied up to the portion that
was more proximal to needle with a second polymer
clip (Figure 4). Afterwards the remained threads that
were inside the cavity were passed longitudinally
through the psoas muscle (Figure 5) avoiding the
genitofemoral nerve, and they were tied as the previous one.
The fixation was tested with the operative table placed
in anti-Trendlemburg position, the hemostasis was checked and a laminar drain was left in the
abdominal cavity.
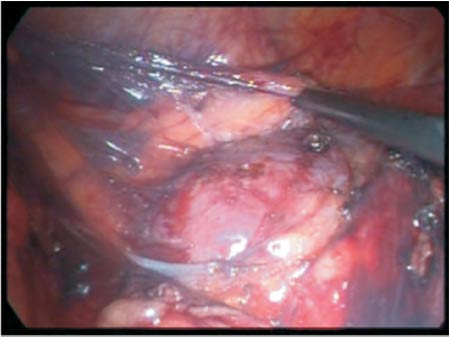 |
Figure 3 - Removal of perirenal fat with Hook clamp. |
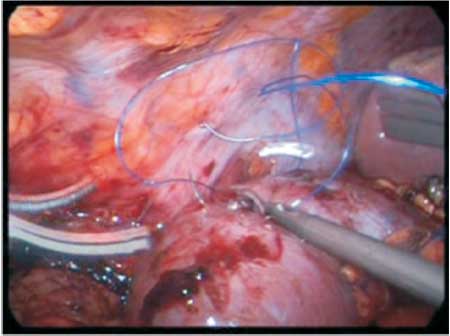 |
Figure 4 - Insertion of the threads through the convex border
of the kidney and its fixation to the lateral of the abdominal wall. |
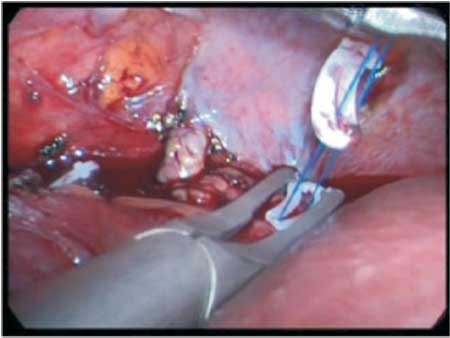 |
Figure 5 - Needle longitudinally passed through the
iliopsoas muscle, in order to avoid the cutaneous branch of the
genitofemoral nerve. |
The operative time was 240 minutes without complications, and an estimated blood loss of 200
ml. On the first postoperative day the oral diet was
started and the drain was withdrawn, patient was
discharged from hospital on the third postoperative day. It
was observed pain and paresthesia since the
immediate postoperative period, tramadol was used to relieve
the pain. Computed tomography was performed before hospital discharge to evaluate the presence of a
hematoma in the psoas muscle which was not
observed. Ten days after the surgery 300 mg of
gabapentin (anticonvulsivant or analgesic for neuropathic
pain) started to be administrated for a month and the
patient is asymptomatic after 3 months of surgery.
Excretory urography depicted the right kidney fixed at L2
level similar to the contralateral kidney. (Figure 6).
 |
Figure 6 - Postoperative excretory urography depicting a
well positioned right kidney without the previous ureteral kink. |
COMMENTS
Open nephropexy which used to be performed indiscriminately in the 70 and 80, has
been abandoned for many years as the outcomes were
not highly satisfactory (in the greatest eight casuistic
it was performed with a 68.6% success
rate2, with 4 to 336 months of follow-up). Add to this fact, the
majority of the urologists were not satisfied with the idea
to perform lobotomy in a procedure that did not have
a good rate of success.
Fornara3 started in 1997 to perform
the procedure via laparoscopic approach (23 patients
only one man and 22 women), with 91% of success
rate and follow-up period of 12 to 27 months.
McDougall (2000) 4 and later
Strohmeyer 5 showed 80% to 76% of success rate, respectively. Some authors as
Hubner and cols. 6 used TVT® to fix the kidney to the
posterior abdominal wall with mesh stapler.
Our option was to perform the procedure without using the mesh, as we do not believe that
this is the most important factor of fixation, and do
believe that a suture well inserted and tied associated
with severe fibrosis which is natural after the perirenal
fat is removed. The greatest casuistic of
laparoscopic retroperitoneal nephropexy did not use mesh in
51 procedures, with a success rate of 91%
improvement in pain and 77% in quality of life, with a mean
follow-up time of 98 months.
In spite of Gozen postoperatively routinely leave the patients in bed rest for 5 to 8 days, we
left only two days due to the fact that computed tomography did not depicted hematomas or
fluid collection. The operative time was 240
minutes because we faced problems with supply of gas
(for 40 minutes), and as this was the first procedure
of this type performed in our Institution.
The idea of not using knot tying initially was due to the necessity of saving time and later we
realize that it was possible to better adjust the suture.
As we did not have the Lapra-Ty® clip we used
Hem-o-lock polymer clip based on previous history of its
use in partial nephrectomy8.
At first it was thought that the pain and
intense paresthesia in dermatome innervated by the
cutaneous branch of the genitofemoral nerve was caused by
the incarceration of nerve due to the suture; however,
as over the period of time the patient only
presented paresthesia, following a neurologist orientation
the administration of an anticonvulsivant (gabapentin)
was initiated as it would act in the neuropathic
pain mechanism. In fact the patient was completely recovered after one month of postoperative,
confirming praxis of the nerve. If within a month there has
not been improvement of the patient's condition, it
would be proposed a new surgery to untie the knots.
COMCLUSION
Laparoscopic transperitoneal nephropexy is feasible, even without using the knot, with
careful attention to the genitofemoral nerve which passes
over the iliopsoas muscle. However, when symptom of
injury in the nerve exists, it could be praxis, and initially
the choice is the clinical treatment of the patient.
REFERENCES
1. Young HH, Davis DM: Malformation and abnormalities
of the urogenital tract. In Young'sPractice of
Urology. Philadelphia, WB Saunders, 1926, pp 18_22.
2. Messias F, Guedes G.A, Argolo R, Fonseca G.:
Nefropexia laparoscópica: Técnicas e resultados In : Mariano
M.B., Abreu S.C., Fonseca G.N., Carvalhal E.F.: Videocirurgia
em urologia;1a Ed Ed Rocca, 2007, p 123-126.
3. Fornara P, Doehn C, Jocham D: Laparoscopic
nephropexy: 3-year experience. J Urol 1997;158:1679_1683.
4. McDougall EM, Afane JS, Dunn MD, et al:
Laparoscopic nephropexy: Long-term follow-up Washington
University Experience. J Endourol 2000;14: 247_250.
5. Strohmeyer DM, Peschel R, Effert P, et al: Changes in
renal blood flow in nephroptosis: Assessment by color
Doppler imaging, isotope renography and correlation with
clinical outcome after laparoscopic nephropexy. Eur
Urol 2004;45:790_793.
6. Plas E, Daha K, Riedl CR, Hübner WA, Pflüger H.
Long-term followup after laparoscopic nephropexy
for symptomatic nephroptosis. J Urol. 2001
Aug;166(2):449-52.
7. Gözen AS, Rassweiler JJ, Neuwinger F, Bross S, Teber
D, Alken P, Hatzinger M: Long-term outcome of
laparoscopic retroperitoneal nephropexy. J Endourol.
2008 Oct;22(10):2263-7.
8. Shalhav AL, Orvieto MA, Chien GW, Mikhail AA,
Zagaja GP, HYPERLINK
"http://www.ncbi.nlm.nih.gov/sitesentrez?Db=pubmed&Cmd=Search&Term=%22Zorn %20KC%22%5BAuthor%5D&itool= EntrezSystem2.PEntrez.Pubmed. Pubmed_ResultsPanel.Pubmed_DiscoveryPanel. Pubmed_RVAbstractPlus"Zorn KC Minimizing knot tying during reconstructive laparoscopic urology. J Endourol.
2008 Oct;22(10):2263-7.
Correspondence address:
Dr. Lessandro Curcio
Av. Ayrton Senna, 1850 / sala 223
Shopping Barra Plaza
Barra da Tijuca - Rio de Janeiro
Tel.: (21) 2430-3257 - Cel.: (21) 9991-9485
Email: lessandrocg@ig.com.br / lessandrocg@hotmail.com